How Big Medicine Can Ruin Medicare for All

Many of us still remember the moment during the debate over the Affordable Care Act when a powerful Democratic senator not only blocked supporters of single-payer health care from testifying before his committee, but even had some arrested. Well, reports are that Max Baucus has been born again. “My personal view is we’ve got to start looking at single-payer,” the now-retired senator recently told a political gathering in his hometown of Bozeman, Montana. “We’re getting there. It’s going to happen.”
Not long ago, politicians advocating for single-payer health care were taken to be on the lefty fringe. But now Democrats of every stripe, including some with plausible presidential aspirations, are using the term to describe what they think America needs now. In 2013, Bernie Sanders couldn’t find a single cosponsor for his single-payer plan, which would replace private insurance with Medicare-like coverage for all Americans regardless of age or income. Today the roll call of supporters for his latest version includes Cory Booker, Kirsten Gillibrand, Kamala Harris, and Elizabeth Warren. Others embrace what they describe as alternative single-payer plans, like Senator Chris Murphy’s legislation that would allow any American to buy into Medicare instead of getting their insurance through their employers or the individual market. It’s enough to make an exasperated Dana Milbank publish a column in the Washington Post under the headline “The Democrats Have Become Socialists.”
But have they? Actually, no. Real socialized medicine, as we’ll see, might work brilliantly, as it has in some other countries. But what these folks are talking about, often without seeming to realize it, is something altogether different. And it could lead to disastrous outcomes unless we get smart about what’s really going on.
Adopting a single-payer system might have done a lot of good—twenty years ago. But since then, a massive wave of corporate consolidations has transformed the American health care delivery system in ways that make the single-payer approach highly problematic. Most Americans now live in places where there is little or no competition among medical providers. In market after market, hospitals, clinics, physician practices, labs, and other key health care infrastructure have been merged into monopolies controlling nearly all aspects of health care in the areas in which they operate.
Switching to single-payer wouldn’t, on its own, address the fact that the lack of competition leaves these Goliaths with almost no pressure to keep costs down. Since medical monopolies are becoming too big for either party to challenge, a single-payer, Medicare-for-all-type plan would likely degenerate into super-high-cost corporate welfare, rather than achieving lower prices or improved quality. The only sure way to avoid that outcome would be to simultaneously enact aggressive antitrust and pro-competition policies to bust up the monopolies and oligopolies that now dominate health care delivery in nearly every community in America.
To see what is really at stake here, we need to begin with a distinction that is typically lost in our health care debates. There is such a thing as socialized medicine, but it’s not synonymous with single-payer. In Great Britain, for example, a socialist government nationalized the health care sector after World War II, and today the British government still owns and operates most hospitals and directly employs most health care professionals.
“A massive wave of corporate consolidations has transformed American health care in ways that make the single-payer approach highly problematic.”
Another example of socialized medicine is the system run by the U.S. Department of Veterans Affairs. The VA owns and operates hospitals and clinics in every state. These are staffed by government employees, most of whom belong to public employee unions. As such, the VA is double-rectified, Simon-pure socialized medicine, even if most members of the American Legion might not put it that way.
Both of these examples of socialized medicine are far from perfect, but they have demonstrable virtues. The UK’s National Health Service produces much more health per dollar than ours, largely because it doesn’t overpay specialists or waste money on therapies and technologies of dubious clinical value. Though they smoke and drink more, Britons live longer than Americans while paying 40 percent less per capita for health care. Meanwhile, a vast peer-reviewed literature shows that the VA, despite dismal press coverage and a few real lapses, actually outperforms the rest of the U.S. health care system on most key measures of health care quality, including wait times and the use of evidence-based medicine. (The health care journalist Suzanne Gordon and I recently wrote a paper for the American Legion, “VA Health Care: A System Worth Saving,” that explores how well VA coverage works.)
For better or worse, what the Democrats marching under the banner of single-payer are advocating is nothing like these examples of real socialized medicine. What they are calling for, instead, is vastly expanding eligibility for the existing Medicare program, or for a new program much like it.
So, what does Medicare do?
It doesn’t produce health care.
Rather, it pays bills submitted by private health care providers.
Thus, under a single-payer, Medicare-for-all plan, the provision of health care itself—its modes of production, if you will—would remain almost entirely in the hands of private enterprise. Meanwhile, its financing would become exclusively a burden borne by government.
The conceptual confusion about Medicare runs so deep that when conservatives call for making the VA outsource its care to private-sector health care providers, liberals generally (and rightly) label such plans “privatization.” Yet these same liberals characterize a Medicare-for-all plan that does essentially the same thing as somehow striking a blow against private control of health care. Meanwhile, many conservatives continue to assert that Medicare is “socialized medicine,” when it’s really the same thing they propose for the VA: a government subsidy for private providers.
So now that we’ve defined our terms a bit better, what can we say a single-payer system would be likely to accomplish? One clear benefit would be to reduce the excessively high administrative costs that weigh down the existing system. Automatically covering every American with a single-payer plan would free up most of the resources that providers and insurance companies currently waste on paperwork and efforts to shift costs to some other player. Patients wouldn’t have to worry about whether the doctor they want to see is “in network” and would avoid a host of other hassles, like having to change doctors every time their employer decides to switch to a cheaper plan.
Having one universal health care insurance plan would also allow the government to stop devoting so much time and money trying to figure out who does or does not meet eligibility requirements for public programs like Medicaid and VA health care. Resources currently spent on sorting out which Medicaid recipients earned too much money to qualify this month, or which of a vet’s maladies are caused by aging and which by his service in Vietnam, could instead go into the hands-on delivery of health care.
The savings could be significant. In 1991, the General Accounting Office estimated that if the U.S. adopted a
Canadian-style, universal single-payer system, the reduction in administrative costs alone would have been enough not only to finance health care coverage for every American, but to do away with all deductibles and co-payments. That’s probably not true anymore. Today, only about 7 percent of U.S. health spending goes to paperwork, largely because the prices of everything else have spiked so dramatically. Still, the U.S. spends a far larger share than other countries on administration, and we could have fixed that a generation ago by moving to single-payer.
We might also have retarded a much more fundamental factor driving health care inflation. Back in the 1990s, single-payer advocates stressed that the real savings would come by giving government “monopsony” power in health care markets. If you are the only buyer in a market with many suppliers—that is, the single payer—that makes you a monopsonist, and it gives you a lot of leverage to negotiate for lower prices. Making government the single payer in health care markets would have allowed it to jawbone doctors, hospitals, drug companies, and medical device makers into charging less and providing safer, more effective health care.
This is what Canada did when it adopted a system in the early 1970s under which each provincial government became the sole purchaser of health care within its own borders. Provincial governments used their monopsony power to negotiate fee schedules with doctors and fixed budgets with hospitals and medical suppliers that left Canadians with a far thriftier, more efficient system. The process was noisy and contentious, but it was carried out in the sunshine and resulted in much lower prices and rates of medical inflation than were occurring in the United States, even as Canadians got greater access to doctors, better health, and longer lives.
So it’s reasonable to think that following the Canadian example twenty-five years ago could have done a lot to restrain health care prices in the U.S. That, in turn, would have made a much bigger difference than most people realize in averting the unsustainably high overall costs of contemporary American health care. That’s because those costs are driven mostly by the prices we pay, rather than by our consuming more care than people in other rich countries.
This is a point worth dwelling on, because it speaks again to how mixed up the terms of debate over health care reform have become. Conservatives often assert that Americans consume too much health care because we don’t pay for it using enough of our own money. Accordingly, they argue that the way to lower costs is to force us to pay more out of pocket through higher deductibles and medical savings accounts, while submitting to narrower provider networks that limit our access to specialists and therefore our consumption of care.
“Not only have sixty drug companies combined into ten, but hospitals and other health care providers are merging vertically and horizontally into giant, corporate health care platforms.”
But it turns out that other advanced countries can offer their citizens universal access to government-financed health care, as well as higher volumes of most forms of beneficial treatment, while still having much lower per capita costs. Canadians see more doctors per year than Americans do while spending about 50 percent less per head on health care. Similarly, the average German is seen by a doctor more than nine times a year, compared to four for the average American. Germans also receive far more hip replacement surgeries per capita and about the same number of knee surgeries, and get to stay in the hospital longer while recovering. Yet the average hospital stay in Germany costs just one-third of what it does in the U.S.
So the big reason why Americans pay more for health care than their counterparts in other rich nations is not complicated. As the health care economist Uwe Reinhardt once put it, “It’s the prices, stupid.”
Most Americans are aware that they pay far more for drugs than their peers abroad. For the thirty most commonly prescribed drugs, prices in the U.S. are roughly double the average for other rich countries. Yet drugs account for only 10 percent of total U.S. health care spending, so they are not the main reason our health costs are so high.
A much bigger factor is the price of physician and clinical services, which account for about a fifth of total U.S. health care spending. Adjusted for differences in the cost of living, the average orthopedic surgeon in the U.S. has a net income nearly three times what France’s equally well-trained orthopedic surgeons make for performing the same procedures. It’s true that many doctors are overworked and underpaid, particularly sole practitioner physicians trying to make a living in an increasingly consolidated sector. Yet the income of the highest-paid doctors, most of whom are specialists and many of whom have substantial investment and business income as well, keeps pulling away. Medical professionals now outnumber lawyers and bankers among the ranks of the 1 percent.
Even salaried doctors are doing well compared to their counterparts in other professions. In the 1980s, an American doctor on salary typically earned about 20 percent more per hour than other American professionals with comparable levels of education. But in recent years, according to a study published in Health Affairs, that income advantage has increased to nearly 50 percent. The McKinsey Global Institute found that if U.S. doctors earned the same amount as their counterparts in other advanced countries, America’s doctor bill would be roughly 35 percent lower.
A still larger factor in driving up costs are the inflated prices charged by hospitals. Hospital care accounts for about a third of total U.S. health care spending. While prices vary dramatically from one hospital to another (depending on how much competition they face), and from patient to patient (depending on their insurance plan), U.S. hospital prices overall are simply astronomical compared to what hospitals in other advanced countries charge for the same services. According to a 2012 study by the Commonwealth Fund, the average hospital visit costs nearly three times more in the U.S. than the average for other advanced countries.
“If you stay in a hospital that faces no competition, your bill will be $1,900 higher on average than if you stay in a hospital facing four or more competitors.”
All this means that if the federal government could use the monopsony power created by a single-payer system to negotiate for more reasonable health care prices, it would be a very big deal. And back in the 1970s, ’80s, and even into the ’90s, something like that just might have been possible. But today, the vast corporate consolidation of ownership in most health care markets in the U.S. makes that a dubious proposition.
Health care delivery in the United States a generation ago was still in many ways a cottage industry. As late as 1995, fully sixty independent drug companies competed in America’s pharmaceutical markets, compared to just ten today. Independent, locally owned pharmacies had not yet been displaced in most communities by giant chains like CVS and Walgreens. More significantly, most doctors still worked as independent sole practitioners or in small group practices. Most hospitals were locally owned, community-focused institutions. In most metro regions of any size, they still faced real competition from other local hospitals over insured patients.
That competition was far from perfect. Regulatory barriers to entry tightly constrained the supply of health care professionals and limited the building of new hospitals. Informal cartels and kickback arrangements between hospitals and doctors were not uncommon. But it was rare for providers to exercise full-fledged monopoly power. In fact, starting in the 1980s and continuing through the ’90s, most found themselves at the mercy of increasingly monopolistic health insurance companies. Doctors and hospitals were put on the defensive as insurers merged with one another and forced providers to make price concessions if they wanted to keep their insured patients. Insurers used their increasing monopsony power to put the screws on drug companies and everyone else in the medical supply chain. This explains why, for a brief moment in the 1990s, the nation’s overall health care bill actually declined.
But then came a counterrevolution that has proven far more consequential. Not only did sixty drug companies combine into ten, but hospitals, outpatient facilities, physician practices, labs, and other health care providers began merging vertically and horizontally into giant, integrated, corporate health care platforms that increasingly dominated the supply side of medicine in most of the country. Like Amazon or Google, these platforms extend their power by controlling the very marketplace in which customers and suppliers have to do business. Even nominally independent surgeons, for example, can’t stay in business if the only hospital in town won’t grant them admitting privileges, or if it grants “affiliated” surgical teams better terms. Many of these platforms became part of large chains operating in multiple regions; others achieved dominance in a single city, which still gave them extraordinary market power.
Local power is everything in health care. Most health care services can’t be imported from China or even from the next county over. Yes, you could drive for hours to see a doctor, or even fly to India or Costa Rica to get an operation, as some people do, but for most people with most conditions that’s not practical. Instead, no matter where you are, most health care is produced and consumed locally, meaning that if providers become organized as a local monopoly it’s a very big deal. In a local market that’s been cornered, even the largest purchasers of health care, including insurance companies and large national employers, become price takers, not price makers.
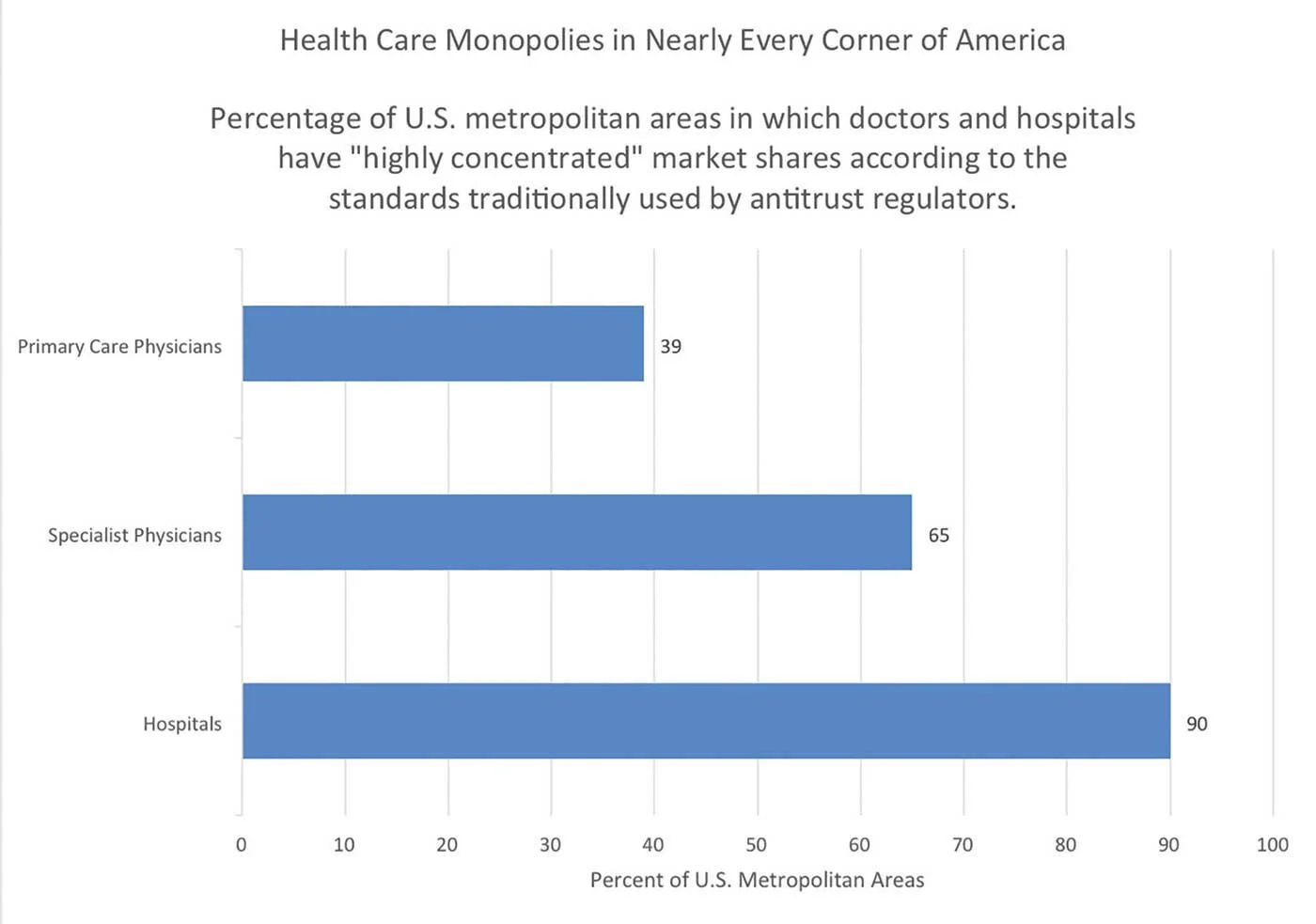
According to a study headed by Harvard economist David M. Cutler, between 2003 and 2013 the share of hospitals controlled by large holding companies increased from 7 percent to 60 percent. A full 40 percent of all hospital stays now occur in health care markets where a single entity controls all hospitals. Another 20 percent occur in regions where only two competitors remain. To use another measure, according to the standard metric used by the Federal Trade Commission to measure degrees of concentration, not a single highly competitive hospital market remains in any region of the United States, and nearly half of all markets are uncompetitive. A study recently published in Health Affairs found that hospital ownership in 90 percent of metro areas is so concentrated that it exceeds what antitrust regulators have historically regarded as the threshold for when action is needed to avoid inefficiency and collusion.
This consolidation in health care shows no sign of abetting. Just the first six months of this year saw fifty-eightmajor mergers among hospitals and health care systems, with six of those involving corporations boasting $1 billion or more in revenue. The absorption of IASIS Healthcare by Steward Health Care, the country’s largest private for-profit hospital operator, will leave Steward with thirty-six hospitals in ten states. This robust merger rate exceeds last year’s. And in 2015, hospital mergers and acquisitions were up by 18 percent over the prior year and 70 percent since 2010.
The effect of this massive consolidation on prices is predictable. According to a study by Yale economist Zack Cooper and others, if you stay in a hospital that faces no competition, your bill will be $1,900 higher on average than if you stay in a hospital facing four or more competitors. The CEOs on top of these chains may be the biggest winners, and it doesn’t matter whether or not the institutions have a “nonprofit” tax status. Toby Cosgrove, the cardiologist who heads the nonprofit Cleveland Clinic, pulled down some $4 million in reportable compensation in 2014.
As hospitals combine into local and regional monopolies, they can leverage their power by buying out local physician practices. Consider the anticompetitive effects of these deals. Doctors play a large role in steering patients to different hospitals, and anti-kickback laws prevent hospitals from paying doctors for these referrals. Yet those laws become inoperative when a hospital simply buys a doctor’s practice and puts him or her on its payroll. Such a deal not only allows a hospital to effectively buy referrals, it also forecloses future competition. To win the business of these referred patients, a rival hospital would generally first need to convince them to change doctors.
The absorption of physicians into monopolistic enterprises is highly inflationary. A 2014 study of physician organizations in California found that groups owned by local hospitals charge 10 percent more per patient than physician-owned groups. Meanwhile, groups owned by multi-hospital systems, which tend to be even more monopolistic, charge nearly 20 percent more per patient. A 2015 study by the National Academy of Social Insurance found that “there is growing evidence that hospital-physician integration has raised physician costs, hospital prices and per capita medical care spending.”
Americans pay for consolidation in other ways. For example, when hospitals in a community merge, one or more often ends up closing its doors, forcing many patients to travel long distances to access the last remaining hospital in their region. Hospital mergers also often result in fewer jobs for nurses and lower-skilled health care workers, in turn eroding their ability to bargain for fair wages and decent working conditions. Though consolidation can sometimes lead to economies of scale and reduce labor costs, the overwhelming consensus of health care economists is that these savings are not passed on to consumers, who instead experience higher prices and lower quality.
So what would happen today if a government program like Medicare were given responsibility for purchasing all health care in the United States? At first it might seem that giving the government that kind of concentrated purchasing power is just what we need to contain the growing monopoly power of hospitals.
But what happens when a single payer finds itself negotiating with a single provider?
If you want a hint at what that would look like, think about how well our “single-payer” Pentagon procurement system does when it comes to bargaining with sole-source defense contractors. Not a pretty picture. In theory, the government could just set the price it’s willing to pay for the next generation of fighter jets or aircraft carriers and refuse to budge. But in practice, a highly consolidated military-industrial complex has enough economic and political muscle to ensure not only that it is paid well, but also that Congress appropriates money for weapons systems the Pentagon doesn’t even want.
The dynamic would be much the same if a single-payer system started negotiating with the monopolies that control America’s health care delivery systems. Think about how members of Congress representing, say, western Pennsylvania would be likely to respond if Medicare-for-all dared to reject the terms demanded by the University of Pittsburgh Medical Center, the region’s dominant health care provider. Notwithstanding its academic name and origins, UPMC is a Goliath that controls nearly 60 percent of the inpatient medical-surgical market in the greater Pittsburgh area.
“In 90 percent of metro areas, hospital ownership is so concentrated that it makes inefficiency and collusion likely.”
Who would blink first if the government threatened to exclude UPMC from its health care plan, which would be the only one available? There are millions of people who live in western Pennsylvania and need access to the hospitals, doctors, and other health care infrastructure UPMC controls. Without access to the system, they might have to drive hundreds of miles to find a doctor or hospital. It would be an instant health care crisis.
Moreover, UPMC is the largest single employer in the Pittsburgh area and one of the biggest in the state. And as it keeps buying more and more hospitals throughout the rest of Pennsylvania, its political power continues to grow. The commercials it would run to get what it wanted from a single-payer system almost write themselves. “The people of Pennsylvania deserve access to the health care they’ve paid for. Tell Congressman Smith to vote no on denying you access to the hospitals and doctors serving our community.”
Of course, in the vision of some single-payer supporters, the government would not negotiate with the likes of UPMC over prices; it would just dictate prices. But it’s unrealistic to expect members of Congress to stand up to corporations that, thanks to unchecked consolidation, not only control the lion’s share of medical professionals and health care infrastructure in their communities, but also are often the largest single providers of jobs and campaign contributions.
Long before consolidation reached the extreme level it’s at today, lobbies for different sectors of the health care system routinely kicked the federal government around. The American Medical Association was so strong that the federal government for years allowed it to set the prices Medicare paid surgeons and other physicians for performing different procedures. Similarly, Big Pharma made sure that the Affordable Care Act contained languageforbidding the federal government from engaging in cost-benefit analysis of drugs, and has dissuaded Congress from allowing Medicare to bargain over drug prices. Similarly, hospital supply cartels have fought off government regulation despite the demonstrably high prices they were extracting from the system. It is frankly naive to expect that health care regulators won’t become even more captured than they already are if the industry they are supposed to regulate gains even more concentrated economic, and therefore political, power.
The choice before us is thus stark. True socialized medicine might work to contain prices and make the U.S. health care system sustainable. But short of flat-out nationalizing America’s health care delivery system, the only other option is to make sure that the market power of hospitals and other providers is sufficiently dispersed that it remains politically possible to regulate them.
Single-payer is therefore doomed to fail unless supporters fuse it with another reform: the aggressive use of antitrust and other competition policies not just to lower drug prices but, even more crucially, to bust up the monopolies that dominate the American health care delivery system. To that end, new legislation would be useful, but even simply leaning on regulators to enforce existing laws would ensure that at least two or three competing health care systems remain in every major metro area. Doing this is not in itself enough to fix America’s health care crisis, but it is a cause to rally around if we are ever to have a sustainable, universal health care system in America.

Subscribe to stay informed.